
Lawmakers in several state legislatures will have a fresh opportunity in 2017 to expand access to oral health care for underserved populations, stretch Medicaid dollars, and liberate dentists to hire a new kind of teammate: dental therapists.
Dental therapists work as members of a dental team, which in many practices also comprises dental hygienists and dental assistants working under a supervising dentist. States that license therapists permit these midlevel providers to perform certain services and minor procedures hygienists may not. These include tooth extractions, restorative treatment, and certain kinds of preventive care. In states that do not recognize the profession of dental therapy, only dentists can perform the kinds of services falling outside hygienists’ scope of practice, which is defined by state law.
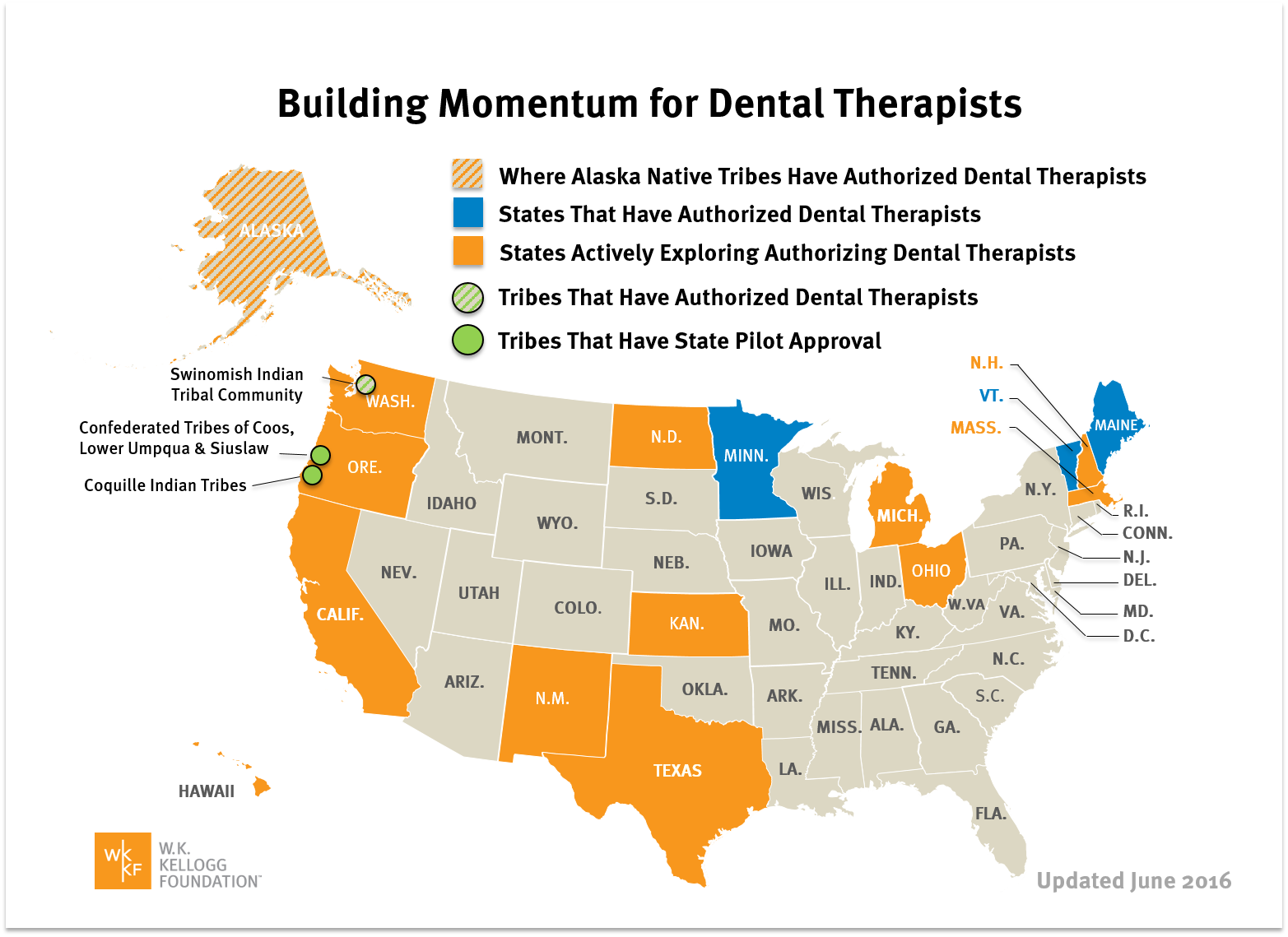
Requirements for education, training, and scope of practice vary among the states where dental therapists are currently practicing: Alaska, Minnesota, Oregon, and Washington. Maine and Vermont permit the licensure of dental therapists, but none currently practices in these states. Approximately a dozen other states have considered or are expected to consider licensing dental therapists in the 2017 session, according to a map published by The Pew Charitable Trusts.
Most states with dental therapy laws require therapists to obtain a master’s degree from a dental therapy program. States are increasingly requiring dental therapists to hold certification as hygienists before entering a dental therapy program, or at least before graduating from one. Although hygienists and therapists typically have different scopes of practice, the availability of dually licensed midlevel practitioners will increase dentists’ flexibility when staffing their practices, in addition to increasing patient access to the level of care they require.
Alaska’s education and training requirements for dental therapists display the flexibility lawmakers of other states have at their disposal. In 2003, Alaska’s program, the first in the United States, was established not by lawmakers but by the Alaska Native Tribal Health Consortium (ANTHC). The program has increased access to oral care for underserved people in an extremely rural state.
In Alaska, to earn one’s license as a Dental Health Aide Therapist (DHAT), a person must graduate from high school, earn an associate’s degree through ANTHC’s two-year educational program, and complete a preceptorship of at least 400 hours under a supervising dentist, according to a state-by-state comparison published at the Vermont legislature’s website. DHATs must also complete 24 hours of continuing education as part of their two-year recertification process.
Alaska’s DHAT program has successfully and safely opened pathways to receiving care for people who previously could not access it. Other state lawmakers can and should adopt a dental therapy program tailored to serve the unique needs of their patient and dentist populations.
Other states, for instance, require at least 2,000 hours of clinical practice under a dentist’s supervision as a condition of licensure. Minnesota also distinguishes “dental therapists” from “advanced dental therapists.” The former holds a degree from a dental therapy program; the latter holds an advanced dental therapy degree and has accumulated at least 2,000 supervised hours of practice.
Opposition to legislation that would allow state health and dental boards to license dental therapists is usually anecdotal at best, illogical at worst. For instance, a Minnesota dentist testified in a hearing of North Dakota lawmakers in September 2016 that his hopes were dashed when the dental therapist he hired required more training and supervision than the dentist expected, which in turn cost the dentist valuable time–his own time and the therapist’s, whose wages were higher than those of the practice’s dental hygienists.
While unfortunate, this dentist’s experience hardly seems representative, considering 95 percent of dental therapists in Minnesota are currently employed, according to data provided by the University of Minnesota School of Dentistry. Owners and operators of for-profit and nonprofit dental and health care practices in Minnesota say employing dental therapists has increased their patient retention rates and even patient satisfaction, Health Care News reported on December 8, 2016.
Dr. Kevin Nakagaki, a dentist at the nonprofit health care organization HealthPartners, says even licensed dentists, whose schooling can last more than twice as long as that of dental therapists, require training and supervision when hired to their first practice. The time investment required training dental therapists is “very similar to managing a new associate [dentist] in your practice, so it gets easy fast,” according to Nakagaki.
Meanwhile, at an average wage of $39 to $46 per hour in Minnesota, dental therapists reduce payroll costs compared to dentists, whose wages average $75 per hour, according to testimony provided to North Dakota lawmakers.
In no state may a dental therapist practice outside of the supervision of a licensed dentist. Dentists who do not want to hire dental therapists will not have to do so if their state lawmakers authorize the licensure of dental therapists.. By no means, however, should a dentist’s right to refuse to hire dental therapists translate to depriving all dentists of their right to do so.
Instead of banning dental therapists from practicing–and depriving dentists of the right to hire them–state lawmakers should approve the licensure of dental therapists as a market-based solution to increasing oral care access for underserved patients.
— Michael T. Hamilton ([email protected]) is a Heartland Institute research fellow and managing editor of Health Care News, author of the weekly Consumer Power Report, and host of the Health Care News Podcast.
IN THIS ISSUE:
DECLINING MEDICAID EXPANSION IN OKLAHOMA IS PROVING A WISE DECISION
During the 2016 legislative session, there was a strong push to expand Oklahoma’s Medicaid program to obtain funding from the Affordable Care Act. Ultimately, lawmakers declined to take that step. It’s proving to be a wise decision.
Supporters of Medicaid expansion argued the costs would be mostly borne by the federal government because Obamacare covered 100 percent of expenses initially, and then at least 90 percent of expansion costs thereafter. But as has often been noted, that law could easily be changed and states could have a greater share of cost burden shifted back to them in the future.
Last week provided a reminder of that fact when President-elect Donald Trump announced that U.S. Rep. Tom Price, a physician and Georgia Republican, would be nominated as Health and Human Services Secretary. Price has called for repealing Obamacare and eliminating the Medicaid expansion, preferring to instead provide tax credits to help low-income individuals buy insurance. For Oklahoma to have embraced Medicaid expansion just as the whole system is being overhauled would have been a logistical nightmare, if not worse.
But even if that were not the case, other states that did expand Medicaid are facing far higher costs than initially estimated. A recent report by the Foundation for Government Accountability notes that expansion enrollment exceeded projections by 322 percent in California, 276 percent in New York, 134 percent in Kentucky, 90 percent in Illinois, 60 percent in Ohio and 51 percent in Arkansas.
That means the cost of the 10 percent state share for Medicaid expansion will be commensurately higher as well. And federal data shows that Medicaid expansion spending was 49 percent higher per enrollee in 2015 than what was predicted when the law passed in 2010.
At the same time, Medicaid expansion isn’t generating the savings supporters promised, such as lowering the use of emergency rooms for routine care.
A study in the New England Journal of Medicine found that Medicaid expansion in Oregon increased ER visits by 40 percent in the first 15 months. …
A side effect of overcrowding in the emergency room is that those with serious medical emergencies wait longer before receiving needed care.
Moreover, Oklahoma already struggles to cover the cost of the existing Medicaid program even without expanding it. …
Should congressional Republicans repeal Obamacare as promised in the coming year, it has been suggested any replacement may include giving states more flexibility to manage Medicaid programs to control costs.
Oklahoma lawmakers would do well to begin devising plans for that possibility and otherwise be relieved they didn’t take the bait on Medicaid expansion.
SOURCE: The Oklahoman Editorial Board
HOUSE APPROVES NEBRASKA VETERANS MED CENTER BILL
The House on Wednesday approved legislation enabling the U.S. Department of Veterans Affairs to work with private donors to build a new $136 million veterans medical center in Nebraska.
The facility, which would be alongside the aging VA Hospital in Omaha, would provide health care services to 175,000 veterans who are living in Nebraska and western Iowa.
Rep. Brad Ashford of Omaha said the legislation “paves the way for major health care improvements” for veterans, including primary health care, mental health care and out-patient surgery.
Ashford, the 2nd District Democratic congressman who was defeated last month in his bid for re-election, said he and Republican Sen. Deb Fischer worked closely together on the legislation. Ashford also gave credit to Republican Rep. Jeff Fortenberry of Lincoln for his efforts.
The groundbreaking legislation paves the way for a public-private partnership in funding the new medical center by authorizing the VA to accept private donations of money, facilities and real property.
Ashford said $56 million in federal funding already has been secured. …
SOURCE: Don Walton, Lincoln Journal Star
INTERSTATE HEALTH INSURANCE SALES HAS A TRYOUT IN GEORGIA BUT NO TAKERS
Among Republican ideas to transform the health care system is a proposal to allow health insurers to sell their policies across state lines.
President-elect Donald Trump and Rep. Tom Price, the Georgia congressman picked by Trump to lead the Department of Health and Human Services, have backed the proposal. They and other advocates see it as a way to boost competition. The interstate sales idea is part of a general GOP blueprint to replace the 2010 Affordable Care Act, often called Obamacare.
In Georgia, the interstate sale of health insurance has already had a five-year tryout.
The state legislature in 2011 passed a bill letting insurers sell any policies in Georgia that they offer in other states. The legislation was hailed by supporters and business groups as a way to skirt the state’s required benefit coverages — such as screenings for cervical, prostate and colorectal cancer, along with mammograms — and thus lower the sticker price of insurance.
The law is still in effect. But since it was passed, no health insurer has taken advantage of it. …
SOURCE: Andy Miller, Georgia Health News
OHIO LEGISLATURE SENDS STRICTEST ABORTION LAW IN THE COUNTRY TO GOVERNOR’S DESK
The Ohio legislature passed the strictest abortion law in the country Tuesday, sending what is effectively a six-week abortion ban to Republican Gov. John Kasich’s desk, in a move that stunned pro-abortion activists.
The bill bans anyone from performing an abortion without checking for a fetal heartbeat or proceeding with the abortion if a heartbeat is detected — usually around the six-week point of a pregnancy. A doctor who breaks the law could be convicted of a fifth-degree felony punishable by up to a year in prison, and could face a civil lawsuit from the mother, reports The Columbus Dispatch. There are no exceptions for incest, rape or health of the mother.
President-elect Donald Trump’s promise to appoint conservative Supreme Court justices to the court emboldened the legislature to move forward with the bill, which was previously stalled over concerns it would be found unconstitutional. Only two other states have passed such a law (Arkansas and North Dakota) and in both cases, the 8th Circuit Court of Appeals declared the law unconstitutional and the Supreme Court declined to hear an appeal to either case.
Kasich has previously opposed the bill over those concerns, but his spokesman declined to comment to the Columbus Dispatch following its passage so it’s unclear whether he will veto the measure. …
SOURCE: Rachel Stoltzfoos, The Daily Caller

Michael Hamilton writes and edits for the liberty-minded clients of Good Comma Editing, LLC, a freelance writing and editing company.




{kind=link}